
Back Pain Guide
A Guide to Conquering Chronic Back Pain Through Science and Self-Experimentation.
Authors: Justin Sterett M.D., Lyndsey Owens D.P.T
Last Updated: 7 Sept 2025
Contents
I. Introduction
It's estimated that 80% of people will experience significant low back pain in their lifetime, making it the leading cause of disability worldwide. Given this incredible prevalence, it's perhaps not surprising that an entire cottage industry has emerged around various programs, devices, medications, and even surgeries aimed at addressing this condition. Yet, despite the immense toll back pain takes on us, nearly 80-90% of cases are labeled "non-specific," highlighting a general lack of understanding or consensus regarding its true causes. Even in medical school, teachings about chronic lower back pain are often limited, tending to focus primarily on surgically urgent or clear neurological issues.
The challenge with the back lies in its complex, three-dimensional structure. It's an intricate system designed to twist, bend, and rotate, featuring multiple layers of muscles and fascia that slide and glide over one another. Within such a dynamic system, the risk of developing imbalances in tension and friction—anywhere along this network—becomes almost inevitable, often leading to discomfort or pain.
I imagine you're reading this because you've experienced, or are currently experiencing, lower back pain yourself. As a physician who treats many patients with chronic lower back pain, I want you to know that I'm right there with you. I believe those best positioned to offer advice are often the ones who've navigated the challenge firsthand. So, I want to share my own story with you.
Click here, if you would rather jump right to the programming.
Around 2016, I began having occasional bouts of mild lower back pain. I attributed these to an irritable Sacroiliac (SI) joint that sometimes felt like it needed to be "put back into place," but otherwise, life proceeded normally. By 2020, however, things started to worsen, and these episodes became more frequent. The bouts of pain lasted longer each time, though I nearly always recovered. Despite this, I remained highly active, participating in CrossFit, Olympic lifting, and even regular yoga sessions. Then, in 2021, while on vacation in the Florida Keys, after a few days of my back feeling "tight," I simply reached down to put on my socks and felt a horrible pinch in the center of my lower back.
Over the next week, I could barely stand. I found myself crawling around the Airbnb just to retrieve ice packs from the freezer. The pain wasn't radicular, meaning it didn't radiate down my leg, so I knew it wasn't a disc pressing on a nerve, and I had no neurological deficits. According to my medical training, this shouldn't have been severe. Yet, it was the most agonizing experience I've ever dealt with. The physical and psychological pain of being unable to bear weight through my axial spine in any direction was truly devastating. At one point, I threw in the towel and went to a local urgent care. Standing upright was almost impossible, and I had to be wheelchaired into the office. I worried I'd be perceived as a typical patient just seeking medication. My X-ray, of course, was normal, and I was given some steroids and pain pills before being sent on my way. Unfortunately, nothing really helped, and sitting on a plane from Florida back to Colorado was one of the most excruciating journeys I've ever endured.
Slowly, over the course of a couple months, things began to improve. I started learning how to use my body again, though even walking any distance felt like a skill that needed to be retrained. It’s important to mention that I was fortunate to have several advantages most people facing this might not. As a doctor, I naturally understood—or at least thought I understood—the anatomy and physiology of my back. I also had the flexibility to control my work schedule, allowing me to take as much time off as needed. Additionally, I had decent health insurance, the financial means, and a general curiosity to explore various treatment modalities to discover what worked and what didn't. This unique position allowed me to truly self-experiment with my back and ultimately led me to share some of these valuable lessons here.
After nearly a year, however, I finally conceded and got an MRI. You don't need to be a radiologist to see something is wrong in the image below; as my five-year-old niece at the time put it, "that looks bad." My L5/S1 disc was essentially non-existent. What likely happened is that for years, I had small tears in the annular ring of my disc until one day it simply gave out. While there are many theories about the pathophysiology of this process, and we still lack a strong consensus on why or how it happens in most people, that was my reality.

Over the last four years, after trying at least a dozen different rehab programs and literally every supplement and "gizmo" on the market, I can report that I've found a balance with my back. I now have far more good days than bad, to the point where most days I don't even think about my back much anymore. It's still a new normal, and coming to terms with what that truly means has probably been the biggest lesson of all.
II. Anatomy of the Lower Back
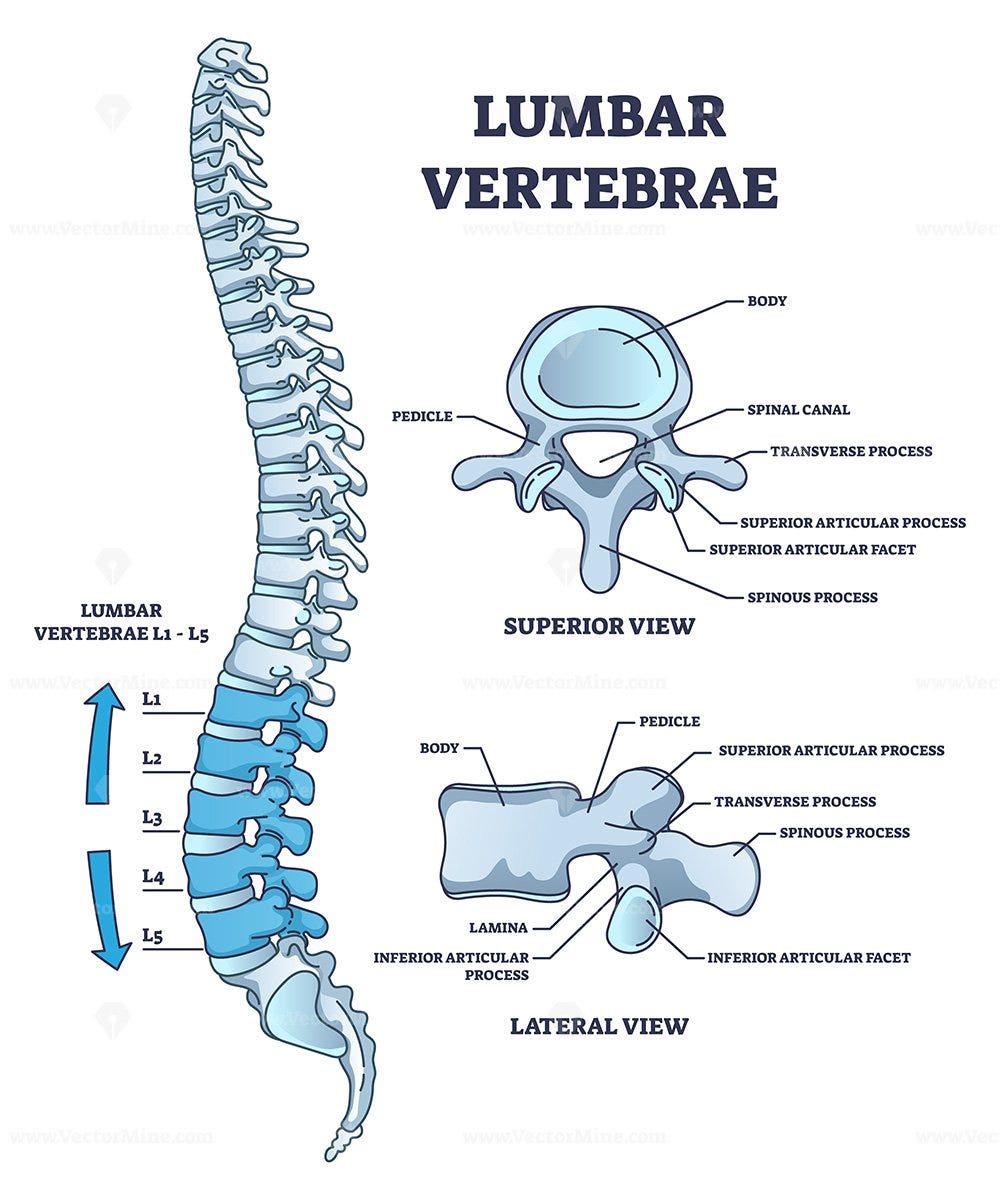
The Lumbar Spinal Column (Vertebrae L1-L5)
The foundation of the lower back is its spinal column, specifically the five lumbar vertebrae (L1 through L5). These bones are distinct from those in the neck or mid-back because they are larger and possess kidney-shaped bodies. This robust design is crucial as the lumbar vertebrae bear the majority of the upper body's weight and efficiently transfer it to the pelvis and lower limbs. Their shorter, broader spinous processes (the bony projections you can feel along your spine) allow for greater movement and provide substantial attachment points for the powerful muscles and ligaments that support this region. Overall, the lumbar spine is specifically designed for stability and flexibility, enabling essential movements like bending, lifting, and twisting.
To better understand the lumbar spine's role, consider it as the root of a tree, prioritizing unwavering support and bearing heavy loads. This contrasts sharply with the cervical spine (neck), which functions more like a thin branch—designed for intricate, highly flexible movements. While the cervical spine's smaller, more delicate vertebrae and highly mobile discs allow for the wide range of head movements we take for granted, they come at the cost of inherent stability. This difference in design means the lumbar spine, though capable of significant movement, is actually less flexible per segment than the cervical spine, emphasizing its role in broad, powerful actions rather than fine, intricate ones. This inherent design also explains why placing heavy loads on the head, such as wearing a bulky helmet for extended periods, can be particularly taxing on the delicate cervical spine, as it fundamentally goes against its design for lighter, more agile movements.
Between each lumbar vertebra lies an intervertebral disc, a vital structure composed of a tough, fibrous outer ring called the annulus fibrosus and a gel-like inner core known as the nucleus pulposus. These discs act as the primary shock absorbers for the spine, cushioning the forces of daily activities, allowing for smooth spinal movement, and maintaining proper spacing between the vertebrae to protect the nerves. Additionally, at the back of each vertebra are paired facet joints. These small, synovial joints guide and limit the spinal column's movement, ensuring stability while still allowing for a controlled range of motion in various directions. Together, the lumbar vertebrae, intervertebral discs, and facet joints form a dynamic and resilient system critical for the function of the lower back.
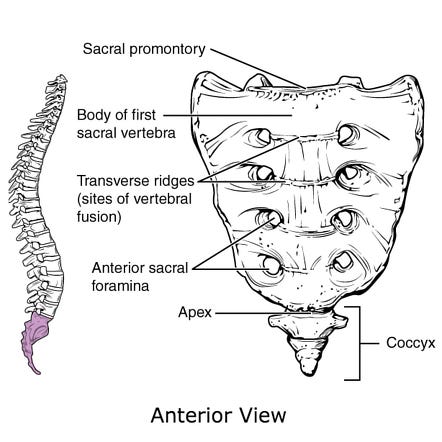
The Sacrum and Coccyx
At the very base of the spine, below the lumbar vertebrae, are the sacrum and the coccyx. The sacrum is a large, triangular bone formed by the fusion of five sacral vertebrae. Its primary function is to serve as a strong base that connects the spine to the pelvis via the (SI) joints. These joints are a key component of the lower back's stability and are crucial for transferring the weight of the upper body to the hips and legs. Unlike the highly mobile lumbar spine, the SI joints are designed for minimal movement, prioritizing stability over flexibility.
Below the sacrum is the coccyx, or "tailbone," a small, triangular bone formed from a few fused vertebrae. While often overlooked, the coccyx serves as an attachment point for several important ligaments and muscles, including those of the pelvic floor, which are essential for core stability.
Muscles of the Lower Back and Core
The muscular system surrounding the lower back is incredibly complex and vital for its stability, movement, and protection. These muscles work in layers, from superficial ones that primarily move the trunk to deep ones that fine-tune vertebral motion. The deep back muscles, such as the Multifidus, are relatively small but immensely important. They span only a few vertebral segments and are crucial for providing segmental stability, controlling individual vertebral movements, and relaying sensory information (proprioception) about spinal position to the brain. Overlying these deep muscles are the more powerful Erector Spinae group. These run vertically along the spine, acting as the primary drivers for extending the back (arching backward) and maintaining upright posture. Another key muscle is the Quadratus Lumborum, connecting the pelvis to the ribs and lumbar spine, playing a significant role in side bending and assisting with hip hiking.
Beyond these direct back muscles, the gluteal muscles (in the buttocks) are critical for hip stability and indirectly influence lower back mechanics. Weakness or dysfunction in the glutes can place increased strain on the lower back. Most importantly, the comprehensive core muscles form a vital cylinder of support around the lumbar spine. This group includes the deep Transverse Abdominis (which acts like a natural corset), the various abdominal muscles, the pelvic floor muscles, and the diaphragm. These muscles work synergistically to create intra-abdominal pressure, which acts like a strong internal brace, significantly enhancing the stability and load-bearing capacity of the lumbar spine. A strong and coordinated core is thus crucial for protecting the lower back from injury and pain.
Equally important are not just the muscles of the posterior chain, but their firing pattern or the precise sequence in which the muscles activate to perform a certain movement. Our bodies move through space because muscles engage in a specific, finely-tuned order. For example, during actions like hip extension (straightening the leg backward or standing up from a chair), the powerful gluteal muscles should ideally fire before the lower back muscles. When this firing order becomes disrupted, such as the lower back muscles activating too early or taking on too much of the load, it can lead to chronic overuse and strain on the lower back structures. Think of it like a car engine misfiring: each component might be capable, but if they don't work in the correct sequence, the entire system becomes inefficient, overstressed, and prone to breakdown.
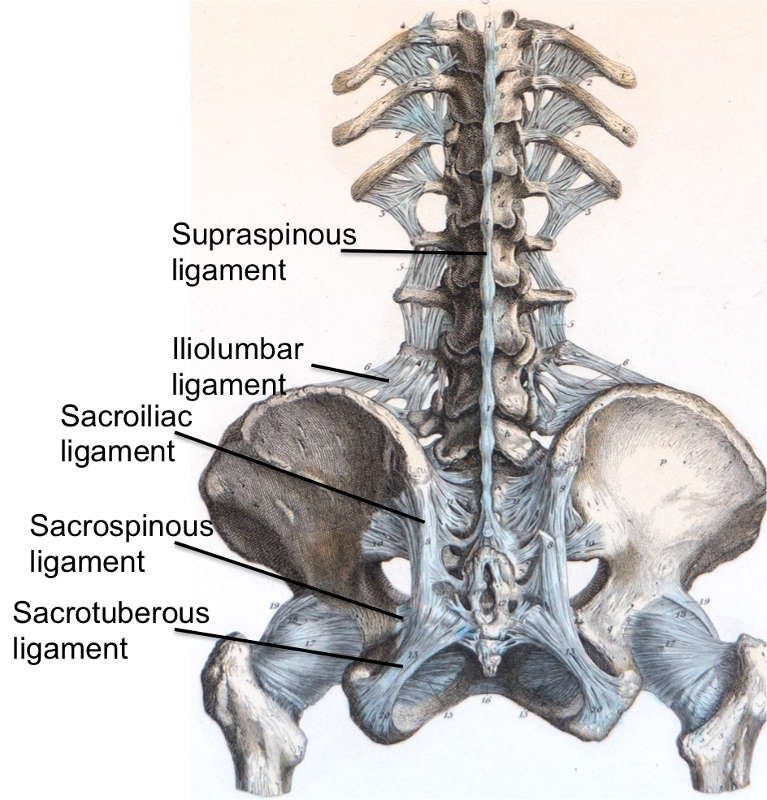
Ligaments and Tendons of the Lower Back
While muscles provide dynamic stability and movement, the ligaments and tendons of the lower back ensure the spine's static structural integrity. Ligaments are strong, fibrous bands connecting bones to bones, providing passive stability and preventing excessive movement. Key examples in the lower back include the Iliolumbar ligaments, which stabilize the L5 vertebra to the pelvis, and the robust Sacroiliac ligaments, which reinforce the connection between the spine and pelvis.
In contrast, tendons are tough bands of connective tissue that attach muscles to bones. Their role is to transmit the force from muscle contractions, facilitating movement and providing dynamic support during activity. Together, this critical network of ligaments and tendons works with the muscles to provide both stability and controlled mobility to the lower back.
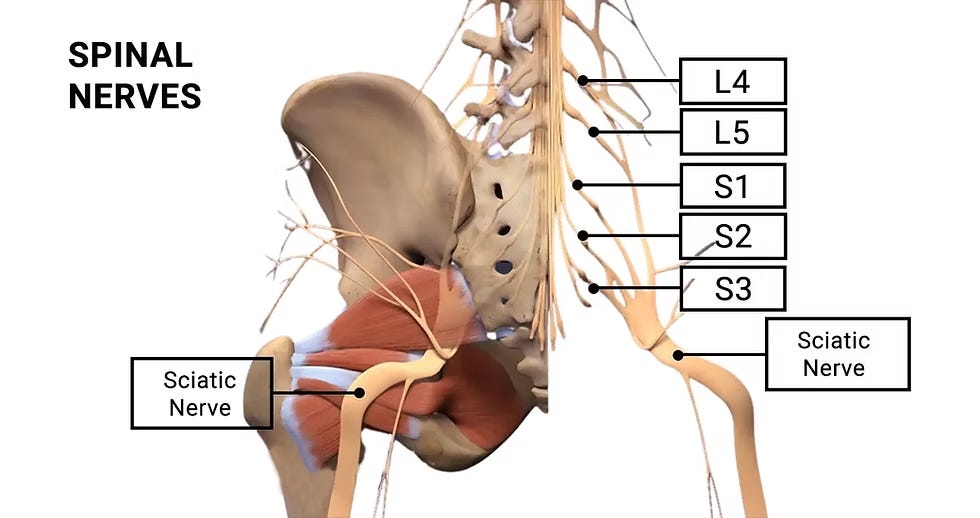
Nerves of the Lower Back
The lower back is a complex hub for nerves that control both movement and sensation throughout your lower body. From each segment of the lumbar and sacral vertebrae, a pair of spinal nerves branches out. These nerves are like two-way communication highways: they contain motor components that send signals from the brain to tell muscles when to contract (allowing for movement), and sensory components that transmit information back to the brain about touch, temperature, and pain from the skin and other tissues.
These individual lumbar spinal nerves (L1-L5) innervate various areas, including the lower back itself, parts of the abdomen, and sections of the legs. The sacral spinal nerves (S1-S5), emerging from the sacrum, primarily contribute to the innervation of the buttocks, perineum, and the legs. Crucially, several of these lumbar and sacral nerve roots then converge to form the Sciatic Nerve, the largest nerve in the entire human body. This thick nerve travels down the back of the leg, providing motor control and sensation to much of the thigh, lower leg, and foot. Any irritation or compression of these spinal nerves or the sciatic nerve itself can lead to symptoms like pain, numbness, tingling, or weakness in the areas they supply. It’s important to keep in mind that general muscle tightness in the lower back and gluteal area can cause compression of some of these smaller peripheral nerves.
III. Causes of Low Back Pain
Understanding some basics of the structure and function of your low back is important to appreciating how normal function can become disrupted.
Back pain, like pain itself, is incredibly complex. Our individual experience and relationship with pain often play as significant a role as the underlying physical mechanisms. While an initial back injury can be temporarily disabling and the physical tissue may heal, the lingering memory and even fear of that injury can persist. This doesn't mean back pain is "all in our head." Instead, our nervous system, through both conscious and unconscious processes, can maintain tension in our system and influence how we experience pain.
Back pain can be understood through two primary frameworks. The traditional biomechanical model states that pain arises from a specific mechanical issue. In contrast, the more comprehensive biopsychosocial model considers not only the biological and mechanical aspects of pain but also the individual's psychological state and the societal and cultural influences that shape their perception and response to pain. Although this discussion, and much of this guide will primarily focus on the biomechanical aspects of injury, it's crucial to remember that pain is a multidimensional experience, shaped by a biopsychosocial framework.
Intervertebral Discs
One of the most common culprits for lower back pain involves the intervertebral discs. Over time, or due to repetitive stress, these discs can undergo degeneration, where they lose hydration and height, making them less effective as cushions. More acutely, a disc herniation (often called a "slipped disc") occurs when the gel-like inner nucleus pushes through tears in the tougher outer ring. When this happens, it can directly press on nearby lumbar or sacral nerve roots, causing localized pain or radiating symptoms. A disc can degenerate and dehydrate without necessarily causing a “herniated disc”, this can still of course be a cause of back pain as the disc itself is highly innervated with nerve fibers and can experience what is known as discogenic pain.
A herniated disc can cause noticeable back pain, but the radiating nerve pain down the leg, often reaching the feet, is frequently more severe. This can also initially appear as leg weakness or neuropathic pain limited to the lower leg. It's important to note that a disc doesn't need to be fully herniated to cause pain; the disc itself can be painful or lead to inflammation in the surrounding vertebrae.

Muscular dysfunction
Muscle pain and dysfunction are also significant contributors. An acute muscle strain can result from overstretching or tearing muscle fibers, often during sudden movements or improper lifting. You might also experience involuntary, painful muscle spasms, which are frequently the body's protective response to an underlying injury or irritation. Furthermore, chronic issues like core weakness can be a major factor; if the deep abdominal and pelvic floor muscles aren't providing adequate support, other back muscles can become overused and strained. Just as important as muscle strength, as previously mentioned is their firing pattern—the precise sequence in which they activate. If, for instance, your lower back muscles are firing before your glutes during a hip extension movement, it places undue stress on the lumbar spine over time, leading to cumulative strain and potential pain.
Tight muscles can also be weak muscles. They should have an appropriate resting firing tone, a "Goldilocks" concept – not too much, not too little. Our posture and movement are determined by how all muscles supporting the skeleton fire at rest. Pain or tightness may stem from a muscle group being outside its optimal resting tone, whether too tight or too loose. When examining lower backs, I always check the paraspinal muscles while the person is standing. People can experience the same type of lower back pain, but some will have very tight paraspinals, while others will feel like Jell-O.
While stretching often provides temporary relief and an endorphin release, allowing shortened muscle-tendon complexes to briefly regain normal length, it's a short-term solution. Without further intervention, such as changes to posture or movement patterns, muscles tend to revert to their deoptimized state, requiring more stretching and perpetuating the cycle. A more effective approach often involves resetting how muscles activate and fire.
Joints and Ligaments
Beyond issues with discs and muscles, the joints and ligaments of your lower back can also be significant sources of pain. Remember, ligaments are the tough, fibrous bands that connect bones and provide stability. If these strong bands, such as those connecting your vertebrae or reinforcing the crucial sacroiliac joints (where your spine meets your pelvis), are overstretched or torn—often from abrupt movements, falls, or trauma—you can experience a ligament sprain, similar to spraining an ankle. This can lead to localized pain and instability.
Another common source of discomfort comes from the small, paired facet joints located at the back of each vertebra. These joints guide and limit spinal movement. However, like any joint in the body, they can become inflamed or degenerate over time, a condition sometimes called facet joint syndrome or localized osteoarthritis of the spine. This often results in localized pain that typically worsens when you extend (arch) your back. Similarly, the sacroiliac joints, designed for robust stability, can also become problematic if they move too much or too little, or if they become inflamed, causing a distinct type of lower back pain.
These joint and ligament issues can sometimes contribute to broader structural problems within the spine. For example, conditions like spinal stenosis involve a narrowing of the spinal canal, which can put pressure directly on the spinal cord or exiting nerve roots. Similarly, spondylolisthesis, where one vertebra slips forward over another, can also compress nerves. Over time, things like bone spurs (small bony growths) or thickened ligaments—often a consequence of degeneration—can further encroach on the space available for nerves, leading to impingement and radiating pain, numbness, or weakness in the legs.
Finally, it's crucial to understand that not all lower back pain originates directly from the spine itself. Sometimes, the discomfort you feel in your back is referred pain, meaning it actually comes from another part of your body, such as problems in the hips, kidneys, or even certain reproductive organs. As you can see, pain in the lower back is rarely due to a single, simple cause; it often stems from a complex interplay of these various anatomical structures and their functions.
Cauda Equina Syndrome: The Urgent Exception-
Cauda Equina Syndrome (CES) is a medical emergency requiring immediate attention to prevent permanent damage. It occurs when the cauda equina, a bundle of nerves resembling a horse's tail at the end of the spinal cord, is severely compressed, commonly by a large disc herniation, but also by tumors, infections, or trauma. These nerves control leg movement, sensation, and bladder/bowel/sexual function.
Key "red flag" symptoms include:
Saddle Numbness: Numbness in the buttocks, groin, and inner thighs.
Bladder or Bowel Dysfunction: Difficulty urinating, loss of bladder/bowel control, or inability to feel a full bladder.
Severe/Progressive Leg Weakness: Difficulty walking, standing, or lifting feet.
Severe Lower Back Pain: Accompanied by other neurological changes.
If these sudden symptoms appear, emergency surgery is crucial, ideally within 24-48 hours, to relieve pressure and prevent irreversible damage like permanent loss of bladder/bowel control, persistent numbness, or paralysis. Prompt intervention is vital for CES, unlike most other back problems.
The Multifaceted Nature of Lower Back Pain
Having explored the intricate structures of your lower back and how they can be affected, it becomes clear that lower back pain is rarely a simple, single-generator problem. Instead, it's often a complex interplay, like a domino effect within a finely tuned system. For instance, in my own experience, when my L5/S1 disc lost significant height, this wasn't an isolated event. It almost certainly led to increased compression and altered mechanics in the adjacent facet joints in my lumbar spine. So, in addition to dealing with discomfort directly related to the disc, I also grappled with facet-mediated pain. This illustrates a crucial point: one change in the lower back often doesn't happen in a vacuum; it triggers other changes, whether they are compensatory adjustments or further degenerative processes, due to the underlying issue.
Given this inherent complexity, isolating the exact cause of someone's back pain can be incredibly difficult, even for the most experienced practitioners. The human body is remarkably adaptable, and pain can manifest in ways that defy straightforward categorization. What's even more important to respect and appreciate is that radiographic imaging, like MRI scans, does not always perfectly correlate with pain and dysfunction. It's a common misconception that every abnormality seen on a scan directly explains a patient's symptoms.
In fact, a now famous 1994 study published in the New England Journal of Medicine found that a significant number of people without any back pain, still had disc bulges and protrusions visible on their MRI scans. This strongly suggests that such findings often reflect normal, age-related wear and tear rather than being the specific, driving factor behind a person's pain. Without a proper understanding of this distinction, a patient may inadvertently overly identify with their radiographic findings, believing them to be the sole cause of their suffering, even when those findings may not be the actual primary driver of their pain experience. This is why a holistic approach, considering symptoms, physical examination, and imaging in context, is always paramount.
IV. Rehabilitation
Finding a solution for back pain is both encouraging and challenging. The good news is that there are several foundational principles that can significantly aid recovery. I'll also share some effective training programs and products that, with consistent effort and proper application, I believe can benefit most individuals. The challenging part is that results vary, and there's no single cure, and likely while all programming has merit, like a diet, the one that works best is probably the one you can stick to, and the one you find benefit in.
As previously noted, the back is a complex 3D structure, and we all place different demands on it, in addition to the psychological factors of pain. Our injury and movement patterns, along with how we interact with them, are unique. Therefore, it's always best to consult an experienced professional for a personalized treatment plan whenever possible.
In this section:
A Paradigm Shift in Back Pain Management
A Paradigm Shift in Back Pain Management
The approach to managing chronic back pain is undergoing a significant transformation. Historically, the conventional medical model has often centered on a passive, reactive framework that can be summarized by the acronym RIPS:
Rest
Injections
Pills
Surgery
While each of these interventions has a defined role in clinical practice, their frequent overuse as first-line or long-term solutions can prove to be a major pitfall, failing to address the underlying causes of the pain. A new paradigm, encapsulated by the philosophy of ATM (Always Treat the Muscles), emphasizes a proactive, patient-empowered strategy that focuses on restoring biomechanical function and muscular health.
The RIPS model has its place, but it is often overused. For instance, temporary rest may be necessary immediately following an acute injury, but prolonged bed rest is not recommended and can be counterproductive. Inactivity can lead to physical deconditioning, creating a feedback loop where lack of movement exacerbates pain, which in turn discourages physical activity. Similarly, interventions like epidural steroid injections (ESIs) and surgery are often considered last resorts or temporary measures. Epidural injections, which deliver anti-inflammatory medication to the spinal nerves, can provide short-term pain relief, but they do not cure the cause of your back pain. Their effects typically last only a month or two, necessitating continued rehabilitative efforts.
Pharmacological interventions, or "Pills," also require a nuanced understanding of their benefits and risks. For acute, severe pain, short-term use of over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, or even prescribed muscle relaxants, can be a valuable tool. This can provide sufficient pain relief to allow a patient to resume daily activities and begin a physical therapy regimen. However, the dangers of long-term reliance are substantial. High doses or prolonged use of NSAIDs can lead to serious side effects, including stomach pain, ulcers, bleeding, and even kidney or liver damage. These risks are compounded by age and pre-existing conditions like diabetes or a history of stomach ulcers. The effectiveness of these medications also has a "ceiling effect," meaning there is a limit to the amount of pain they can control, regardless of dose. The most serious concerns are associated with narcotics, or opioids which outside of the most extreme acute cases should not be given for back pain.
Mechanical back pain is often a direct result of improper biomechanics, which may involve muscle strains, weakness, and poor movement patterns. Therefore, addressing the underlying muscular and postural issues is a necessary long-term solution. A shift towards a proactive model that targets the root cause—the muscles and their function—offers a more comprehensive and ultimately safer pathway to lasting relief.
Physical Therapy 101
Having spent considerable time with physical therapists and exploring various programs for my own back pain, I've identified a core rehabilitation principle taught to me by a brilliant DPT that holds true for both acute and chronic pain. This principle can be applied to any movement system in the body, not just the back, and can be structured into a six-step approach. It’s worth noting and keeping in mind before we move through program recommendations. Most effective programs for rehabilitation are built on these principles in one way or another.
Start with pain modulation
Identify restrictions in soft tissue or passive structures
Reduce sensitivity through manual therapy or other calming therapies.
Load local tissues
Once neuromotor tonicity or passive range of motion is improved, retrain tissues to recognize, accept, and apply force appropriately.
Progressive loading depending on stage of recovery to increase capacity for functional tasks and training.
Integrate into the full kinetic chain
Move beyond isolated tissue to coordinated, global movement patterns.
Ensure the body works as a system, not just individual parts
Challenge proprioception and kinesthesia, addressing each plane and combination of planes of movement as appropriate for patient specific demands.
Train energy storage and release
Add plyometric and power-focused work once foundational strength is built.
Reflect how life actually works-short bursts of power and quick reactions.
Reject “fake functional” exercises
Instead of mimicking arbitrary tasks (e.g., lifting a laundry basket in one plane of motion with perfect deadlift form) focus on meaningful, transferable movement patterns.
Recognize overlap between stages
Patients are often in multiple stages at once.
The process isn’t perfectly linear–loading chain integration, and power development often blend together.
These six concepts apply to both acute and chronic issues. People often feel stuck months or even years after an acute injury that does not seem to be improving, or keeps getting re-injured. Should pain persist without measurable/perceptible change, in addition to the above concepts it’s worth considering the following for most chronic pain
:
The underlying cause of the injury has not responded to modes of intervention.
Not all nervous systems respond in a predictable manner. Depending on the chronicity of the pain and the various biopsyhosocial factors surrounding the injury and recovery, the robustness of response will vary and prognosis will be impacted.
There is possibly a new structural reality to our back that has led to a new normal of how to exist with our backs to stay out of pain that we simply fail to either understand or respect.
Program Specific Training
Before diving into this section, I just want to note that it is dynamic, and constantly being updated. It’s also worth stating that although I have found benefit in the programming below, there is no one-size-fits-all solution. As mentioned before, the programming that works best for you is likely the one you can stick to, and most importantly, is working. As you begin this journey to heal your back, understand there are more types of programming out there than there are hours in the day. You can’t do everything at once, and this will require a bit of self-experimentation.
Generally speaking, I’ve tried to put these in order of my experience and my patients’ experiences of their effectiveness. When possible, I’ve also mentioned when in the rehab process I think they should be applied. I’ll provide a brief overview and some links but consider these an introduction and not a comprehensive overview.
1) Dr. Stuart McGill, and the McGill Big Three
Dr. Stuart McGill is a prominent back pain expert and former professor at Waterloo University, he has dedicated three decades to researching back pain, rehabilitation, injury prevention, and performance enhancement in his lab and clinic. His work has significantly advanced the understanding of back injuries and the vital importance of core stability. His work underscores the body's intrinsic need for precise muscle and joint coordination, particularly within the "core" musculature that envelops the spine. McGill defines spinal stability as a two-fold concept: stiffness, which refers to the muscles' capacity to generate force and bear external loads, and linked system function, where movement in the extremities necessitates proximal stiffness in the core. A deficiency in core stability, according to McGill, is a primary precursor to various back injuries.
While many fitness regimens favor dynamic exercises, McGill strongly advocates for isometric exercises as a superior method for enhancing core stiffness and stability. This preference stems from the fact that isometric movements focus on muscular endurance and coordination without involving significant joint motion, thereby aligning perfectly with the core's fundamental role: to limit excessive spinal movement and facilitate the efficient transfer of force throughout the body.
Effective core stability training, McGill emphasizes, involves the co-contraction of all core muscles. This integrated approach, often likened to creating a "natural weightlifting belt," is far more effective than attempting to isolate specific core muscles. Research, he notes, demonstrates that true isolation of these muscles is not only impossible but also less efficient than a bracing strategy that engages the entire core unit.
For back injury rehabilitation, McGill developed "The Big 3" exercises: the Curl-Up, Side Plank, and Bird-Dog. These exercises were selected after extensive laboratory comparison of numerous alternatives. There is a very specific way and cadence to performing these movements that is critical to their execution.
The big three exercises are recommended for daily performance, though it's crucial to avoid doing them immediately after waking due to increased spinal disc hydration in the morning, which can make the discs more vulnerable. Beyond targeted exercises, regular walking is also highlighted in the McGill methodology as a highly beneficial activity for spinal health.
To dive deep on the McGill methodology I highly recommend his book Back Mechanic, which provides comprehensive strategies for managing back pain, and Ultimate Back Fitness and Performance, which offers guidance for continued progress and optimizing athletic function.
2) Foundation Training: Dr. Eric Goodman
Created by chiropractor Dr. Eric Goodman, the method grew out of his personal journey to find a solution for his own debilitating back pain, which at one point was so severe he was advised to undergo spinal fusion surgery. Rejecting that as his only option, Dr. Goodman dedicated himself to understanding the body’s natural support system, specifically the posterior chain muscles—the interconnected muscle groups running along the back of the body. He realized that strengthening and properly utilizing these muscles could provide a powerful, lasting solution to chronic pain.
Foundation Training combines mindful movement with specific breathing exercises to teach your body how to move more efficiently and correctly. It goes beyond treating symptoms by addressing the root cause of many physical imbalances that arise from our modern, often sedentary lives. By strengthening your body’s foundation, you can regain control of your movement and build a more resilient physical state.
What is Foundation Training and How Does It Work?
Foundation Training teaches the body to move with strength and stability using unique exercises based on core principles.
Decompression Breathing: A central element of the practice is a specific type of breathing that creates length and space within the spine. This "decompression breathing" helps to counteract the effects of gravity and poor posture, which can compress the spine over time.
Strengthening the Posterior Chain: The exercises are designed to activate and strengthen the muscles of the posterior chain, including the hamstrings, glutes, and back. This focus on the body’s natural support system helps to reduce the strain on the spine and correct imbalances.
Movement Integration: Instead of isolating individual muscles, Foundation Training teaches the entire body to work as a unified unit. This creates efficient movement patterns that reduce stress on joints and tissues.
The Founder Exercise
The Founder is the signature exercise of Foundation Training and is considered one of its foundational movements. It teaches proper hip hinge mechanics and engages the entire posterior chain to help alleviate pain and improve movement patterns. To perform the Founder, you stand with your feet hip-width apart and bend forward at the hips, keeping your knees slightly bent. Your arms reach straight out in front of you, and you hold the position for several breaths, engaging your glutes and hamstrings to help lift you back to a standing position. This exercise reinforces correct movement and assists with spinal decompression, making it a powerful tool for building foundational strength

Foundation Training takes a broader, more general approach. Instead of just focusing on building core stability like the McGill methodology, it teaches the entire body how to move better to reduce pain and build long-term resilience. Foundation Training focuses on integrating the posterior chain and breath into all movements to support the spine, creating a foundational strength that applies to all aspects of life, from lifting objects to sitting at a desk.
While it was a difficult choice, I've placed Foundation Training after the McGill Big Three. Foundation Training is the program I most frequently recommend, and it has consistently yielded more positive outcomes for individuals than any other method I've suggested. However, when I initially began doing this I found my lower back lacked the necessary strength to keep up. For me, several months of consistently performing the McGill Big Three were essential to build the stamina required to effectively engage in Foundation Training; thus, the sequence was crucial.
The most effective way to begin Foundation Training is to subscribe to FT streaming and commit to the beginner daily workout routine for several weeks. This approach offers a structured, progressive sequence that will teach you all the necessary fundamentals. Alternatively, you can try the popular 12-minute YouTube video, though it's advisable to review this free ebook supplement first, as it explains some of the core principles.
3) Kinstretch
Kinstretch is a movement system developed by Dr. Andreo Spina, the founder of Functional Range Systems (FRS). Unlike traditional stretching, which primarily aims to lengthen muscles, Kinstretch focuses on building functional mobility and joint resilience. The system is based on scientific principles and is designed to improve your body's ability to control its full range of motion.
Kinstretch is a unique practice that prioritizes active control over passive flexibility, despite the name it is anything but simple stretching. The core philosophy is that true mobility is not just about how far you can move a joint, but how much control you have at that joint's end range of motion. The system employs two main types of exercises:
Controlled Articular Rotations (CARs): These exercises involve actively moving a joint through its largest possible pain-free range of motion. CARs help to maintain joint health and provide a daily assessment of your mobility.
Progressive and Regressive Angular Isometric Loading (PAILs/RAILs): These are isometric exercises performed at the end ranges of a joint's motion. PAILs involve contracting the muscles that move you into the stretch, while RAILs involve contracting the muscles that move you out of the stretch. This method effectively builds strength and control in your deepest ranges, where injuries are most likely to occur.
Kinstretch aims to build a more robust and adaptable body by expanding and strengthening your usable range of motion. This proactive approach helps prevent injuries, as it specifically trains the body in the "odd positions" where most injuries occur.
Consider nearly every injury you've experienced; it likely happened at a joint's end range of motion and in an unusual position. These are body positions most of us rarely train in and are generally susceptible to injury.
While I generally recommend introducing Kinstretch later in the rehabilitation process for acute injuries, it's the one training method I wish I had started two decades ago. I've found Kinstretch to be incredibly effective. For instance, a few years ago during a deployment, I urgently needed to retrieve gear from a shed while wearing body armor. The required box was beneath an awkwardly shaped fuel safe, labeled 130 pounds. I couldn't get into a good lifting position and was forced to lift it with a slightly flexed spine and too far in front of me. I vividly remember thinking, "When I'm in a wheelchair months from now, this will be the story of how I got there." However, I lifted the safe, twisted, and safely set it down. I was slightly shocked that I was okay. Throughout most of that deployment, I was doing Kinstretch every other day, specifically training end-range of motion lumbar flexion drills. I truly believe it saved my back that day.
There are likely many entry points into Kinstretch, but the programming I found that I still use today was developed by Amir Zanedinejad. Amir has really doubled down on the marketing of his epic beard and his website can be found at www.beardthebestyoucanbe.com. There is a free class to try on the landing page, and the monthly subscription to his content is on the higher side, but the benefit to a subscription is not only getting access to his 200+ plus classes, but that he will personally work with you in a private forum to develop custom routines for your needs.
4) Core Balance Training
Core Balance Training is an online program developed by Dr. Ryan Peebles, a Doctor of Physical Therapy who spent over 20 years researching and reversing the root causes of chronic lower back pain after suffering from it himself for a decade. The program is a unique movement retraining system designed to treat back pain in just 15 minutes a day. It focuses on teaching individuals how to heal the body from within by addressing the source of the problem, not just the symptoms. For this reason, it is an excellent resource for early rehabilitation, helping individuals learn how to breathe and move again, but really it is for anyone with chronic pain as well.
Core Balance Training aims to correct fundamental muscular and postural imbalances that lead to chronic pain. The program's core philosophy centers on the idea that many people's chronic pain stems from the body's inability to properly utilize and stabilize the deep core muscles. Instead of relying on crunches or sit-ups, it teaches people how to engage their core to support their movements. The training's principles include:
Movement Retraining: The program teaches you how to change movement patterns that contribute to pain. This involves learning to properly engage deep core muscles to transfer power from the core to the limbs, rather than relying on the limbs alone.
Holistic Approach: The training focuses on overall health, posture, and the relationship between the body and mind, aiming to improve not only physical pain but also quality of life.
Small Patterns: Core Balance Training emphasizes neuromuscular retraining and proprioceptive patterns, differing from general strength and conditioning. Unlike programs like Foundation Training and Kinstretch that focus on strength and mobility, Core Balance corrects unconscious movement patterns causing pain by retraining deep core muscles and the body's internal support system, focusing on movement quality over lifting capacity.
The program is designed to be progressive and accessible to all ages and fitness levels. It consists of 12 modules that gradually build upon each other, with the first module focusing on teaching proper core engagement as a foundation before moving to more complex movements. It’s another pricey subscription based plan, but I found that all you need is to run through it once and then be done with it.
Notes on stretching
My views on static stretching have evolved considerably over the past few years, a sentiment shared by many physical therapists. It's widely recognized that tight muscles are often weak muscles. While stretching might offer temporary relief due to endorphin release from tissue elongation, it doesn't address the underlying issue of weakness.
However, stretching still offers significant benefits. It can be incredibly relaxing and serves as an excellent opportunity for self-awareness. Many general movement dysfunctions stem from a disconnect with our bodies. Incorporating deep breathing into long-hold static stretches is not only a way to reconnect with your body but also to begin calming an overstimulated nervous system.
The 20-30 second stretches learned in high school sports are likely insufficient. Research indicates that stretches lasting upwards of two minutes are sometimes necessary to truly engage deep neuromuscular tissue.
For an effective stretching program that incorporates these longer holds, I recommend Pliability.com.
Honorable Mention
Although I’ve never tried this program it seems to have helped a lot of people online. The core tenets of the program include a focus on progressive overload, improving hip and upper back mobility, and direct low back ability training, all while encouraging members to avoid the "avoidance mindset" that often accompanies chronic pain. So fundamentally very similar to programming listed above. To learn more check out this AI generated deep research report on it, or the podcast they run.
Equipment
I confess, with a mix of pride and embarrassment, that my collection of foam rollers, myofascial release balls, and other peculiar, torture-device-like tools could easily compete with a well-stocked physical therapy clinic. While a comprehensive review of these items—what's effective and what's merely marketing hype—deserves its own e-book and is beyond the scope of this guide, I felt compelled to highlight a few items that I can’t live without. These select few will always find a place in my travel bag, even when I'm packing minimally.
Shakti Mat
This is an acupressure mat that has become popular in recent years. It is made up of thousands of plastic spikes that are harmless, but firm and sharp enough to activate similar principles of acupuncture and acupressure. I feel that this mat has several mechanisms of action for not just back pain, but overall wellness and even mental health.

Muscle Relaxation: Laying on one of these mats initially shocks the system, but the pressure from the spikes aids in releasing back muscle tension through sensitization. After 5-10 minutes, you'll begin to relax, and your muscles will actually become less tense than before you started. My back is normally tight every morning, and this is the first thing I do each day for 10 minutes.
Endorphin Release: Lying on the mat can trigger the release of endorphins and oxytocin, the body's natural pain-relieving hormones. This can lead to a sense of relaxation and well-being, helping to reduce the perception of pain.
Mind-Body Connection: The intense sensation requires a certain degree of mindfulness to endure, which can help draw attention away from the pain and into the present moment. This can be a form of active meditation that helps with pain management.
They also offer a neck pillow that can be used with the mat to help desensitize an irritable neck.
Inflatable Lumbar Travel Pillow
The McGill Methodology also supports this idea. For those who travel frequently and are obliged to use public transportation, you'll notice that airline seats seem designed for a "C"-shaped spine, not an "S". I always bring an inflatable lumbar pillow. One observation I've made is that when my disc collapsed, it heavily impacted my facet joints. For instance, bending backward and lying flat are difficult as they extend these joints. While it may seem counterintuitive, providing extra lumbar extension support while sitting actually helps decompress the facet joints.
Final Thoughts
Back pain is unfortunately a problem many of us will have to live at some point in our lives. While the odds may seem against you, back pain doesn't have to dictate your quality of life. There is hope for those struggling, but it often requires accepting new normals and making significant changes to your relationship with your body.
My own four-year journey with back pain has had its share of ups and downs, but the goal is to achieve more good days than bad. I am incredibly grateful for the insights I gained about my body during this healing process. I discovered strategies that not only helped my back but also improved my overall joint and physical health. True back healing is a holistic journey that involves caring for your entire system.
I hope this guide has been helpful. I recognize that I haven't covered topics like nutrition and dietary supplements, but the guide is constantly being expanded with updated topics and new information.
Aeromedical
This section is tailored for aviation professionals, examining how both the USAF and FAA occupational medical standards address back pain.
USAF
Pilots and aircrew face a unique challenge regarding back pain due to the demands of their flying duties. Prolonged sitting, combined with shifting G-forces and axial spine stresses, creates a high-risk environment for developing back pain. Despite this, many aircrew members are reluctant to report these conditions to medical personnel, fearing it could lead to grounding or require a waiver to continue flying. Consequently, chronic back pain often goes unreported and unmanaged. This section aims to provide essential education on Air Force standards to encourage seeking care without jeopardizing one's career.
Aeromedical standards for individuals on flying status focus on two main areas: significant impairment and radiographic evidence of specific conditions.
Any musculoskeletal condition affecting the spine or extremities that impairs duty performance, restricts deployments, or persists despite treatment necessitates a waiver for both continued flying duties and military retention. While minor medical standards exist specifically for aircrew (e.g., not requiring an external brace for ongoing back pain), subjective back pain generally doesn't require a flying waiver if it doesn't hinder job performance or lead to frequent absences.
Flight surgeons often have considerable discretion in interpreting back pain, especially if it doesn't overtly restrict duties. While a waiver may not be necessary for a specific condition, a pilot could be temporarily grounded if there's a concern that the pain might become severe enough to distract from or impede aircraft egress.
Conditions exist where a waiver for flying duties is mandated solely by radiographic findings, even without clear clinical correlation. This underscores my view against unnecessary imaging: it's not just wasteful, but incidental findings can force a flying waiver. While imaging is important, as noted elsewhere in this guide, it often doesn't correlate with clinical findings. I typically consider advanced imaging only when it will inform a clinical approach, usually when surgery is already a consideration, or the etiology of the pain is not clear.
A common reason for an aircrew member to require a waiver due to imaging findings is a history of a herniated nucleus pulposus, or a disc herniating or bulging through its wall, or surgery for this condition. This is a valid concern due to the risk of sudden exacerbation, especially in high-performance aircraft, and the potentially lengthy recovery time for surgical fusions and similar procedures. In some instances, a waiver may still be necessary even if the finding is incidental or potentially old. In a review of waivers in 2019 the waiver success rate for this condition was as followed: FC I/IA (38%), FC II (93%), FCIII ( 84%).
FAA
The FAA evaluates spine and back issues based on how they affect a pilot’s ability to safely operate an aircraft. This includes maintaining control of the plane, handling emergency situations, and tolerating the physical demands of flying. Examiners are trained to look for signs that a pilot may have difficulty with mobility, balance, or endurance.
Simply having a history of back pain doesn’t mean you’ll lose your medical certificate. The key questions are: Is the condition stable? Does it interfere with flying duties? Are you on medications that could impair cognitive or motor function?
Conditions You Can Usually Fly With
The FAA has a program called CACI (Conditions AMEs Can Issue) for certain stable conditions that previously required FAA review. If your back condition falls into one of these categories, your Aviation Medical Examiner (AME) can issue your certificate at the time of the exam, as long as specific criteria are met. Examples include:
Chronic Low Back Pain: If your back pain is stable, not disabling, and not treated with disqualifying medications (like opioids), you may qualify for CACI issuance. The AME will need documentation of stability and treatment.
Scoliosis: Stable, non-progressive scoliosis without neurologic involvement or significant functional limitations can often be handled under CACI.
Degenerative Disc Disease (mild cases): If there’s no neurologic deficit, no recent exacerbations, and no recent surgery, this may be managed without FAA deferral.
These conditions require the AME to complete a worksheet verifying that your status meets FAA standards. If you meet all the criteria, you may be issued on the spot.
When You’ll Likely Be Deferred
Some spinal conditions, however, require deferral to the FAA for further evaluation. These usually involve higher risk of sudden incapacitation or functional limitation. Examples include:
Herniated Nucleus Pulposus (HNP): If you’ve ever had a herniated disc—especially one that caused radiculopathy or required surgery—the FAA requires a detailed review. Even if you're asymptomatic now, the history alone typically results in deferral.
Spinal Surgery: Procedures like spinal fusion, disc replacement, or laminectomy almost always require FAA review, along with post-op imaging, a neurology or orthopedic report, and functional status documentation.
Use of Disqualifying Medications: Chronic use of narcotics, muscle relaxants, or medications that impair alertness are generally incompatible with flight duties and will trigger deferral.
What You Can Do
To reduce the risk of complications in certification:
Disclose honestly, but be prepared: Bring documentation from your treating provider describing your diagnosis, treatment, current function, and prognosis.
Understand medication rules: Over-the-counter NSAIDs are generally fine. Opioids, benzodiazepines, and some neuropathic pain meds can be disqualifying.
Don’t delay care: The FAA’s evolving approach focuses on returning pilots to flying safely—not punishing them for seeking help. Getting care early and documenting recovery may actually speed up your return.
Bottom Line
The FAA’s goal is to ensure that all pilots are fit to fly—not to ground them unnecessarily. Many spinal conditions, including back pain, are manageable within the system. Knowing which conditions are routinely issuable and which require further review can help pilots make informed decisions about treatment and disclosure. When in doubt, ask your AME early—there may be a clear path forward, even with a complex medical history.